|
|
|
|
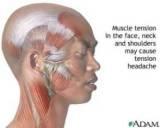
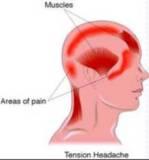
Tension-Type HeadachePathophysiologyExtracranial muscle tension Questioned relationship Muscle tension is cause or epiphenomenon Common pathophysiology with migraines and represent different ends of a clinical spectrum
Clinical FeaturesBilateral, nonpulsating, not worsened by exertion, not ass with N/V
In severe cases --> fit the description of mild migraine
Accurate classification requires at least two of the following four characteristics:
Important associated symptoms include
Typically nausea and vomiting do not occur. TreatmentSimple analgesics or NSAID Same as migraine in severe cases
Cluster HeadacheEpidemiologyRare (0.4% prevalence rate) Very short-lived even without treatment More common in men Onset after 20 YO PathogenesisDysfunction of the trigeminal nerve A common mechanism with migraines (respond to 5-HT 1D agonist)
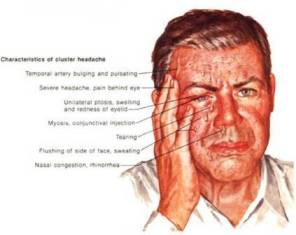
Clinical FeaturesVery severe, unilateral or bital, supraorbital, or temporal pain Lasting 15 to 180 min Pt rarely lie still, most are pacing and restless Clinical FeaturesIt generally lasts forty-five to sixty minutes. There is no associated aura. Associated features include
There is often a history of excessive alcohol intake and heavy smoking. Tend to occur in “cluster”
TreatmentOxygen : Effective up to 70% DHE and Sumatriptan NSAIDs : Reducing the frequency and severity of future attacks Oral agents are unlikely to be effective (short duration of Dz)
Disposition for All Primay Headache SyndromesPoor response --> suspect secondary cause and prompt emergent Ix Respond well --> D/C and F/U Intractable migraine --> admission for more aggressive pain control
Summarized By Thirayost Nimmanon â´Â ¸ŐĂÂĘ¶ě ąÔÁÁŇąą·ě
|
|
»ĂŃş»Ăا¤ĂŃé§ĹčŇĘŘ´ 15/06/2010
ä´éĂŃşˇŇĂʹѺʹع Web Hosting ¨Ňˇ SPAComputer.com, ThaWang.com |