|
|
|
|
Sensorineural Hearing LossCaused by a disorder of the inner ear,cochlea,or VIII nerve Range from mild to total,ie,greater than 120 dB HL Nerve deafness or nerve loss
EtiologyDevelopmental & Hereditary disorder
Toxic nerve deafness
Infectious disorder
Trauma
Meneire’s disease (Endolyphatic hydrops)Central origin (Multiple sclerosis)Bone disorder (cochlear otospongiosis)Neoplesm (acoutic neuroma)Endocrine (DM, congenital hypothyroid , hyperthyroid, hyperlipidemia)disorder of unknown etiology(Presbyosis)Others : vascular, immune disorder, renal, psycologic deafness)
Developmental & Hereditary disorderCongenital nerve deafness c loss at birth
Hereditary nerve deafness
Clinical : FH+, delay speech, G&D
High-risk Indicators of Hearing Loss : Birth to 28 days
High-risk Indicators of Hearing Loss :29 days to 24 months
Toxic nerve deafnessMost often found in childhood post acute febrile illness stage of severe general infection eg. Measle, scarlet fever, influenza, pneumonia etc. Typical Hx: normal hearing->sudden loss Usually bilateral high frequency symmetrical and spontaneous(normal) resolution
Pharmacologic toxicityAminoglycosidesmost common caused, usually c nephrotoxic Almost cochleotoxic (hair cell damage )> Vesibulotoxic except steptomycin & gentamicin) Antimalarial :SHNLQuinine : tinnitus, nausea, visual-> “Cinchonism” Chlroquine:macular degeneration Large dose may be permanent HL Salicylateshearing return to normal in 72 hr
Infectious disorderCongenital Syphilis n. deafnessRapid progressive asymetric SHNL+/- vestibular symptom occurring several to many years after chidhood interstitial keratitis Hx,serology,VDRL,FTA-Ab Rx:2sy benzathian PGs 2.4 mU IM,3 month c prednisolone40-80 mg/d daily then decrease 10 mg q 2 day Aquired syphilis n. deafnessoften in late tertiry Sy positive blood serology Rx PGS IV Labyrinthitis (serous/supperative)Unilateral depression of cochlear function c vertigo and diplacusis Young and middle aged Recovery depends on severity Serous labyrinthitis : secondary to ASOM or CSOM or surgical trauma Supperative : with infection
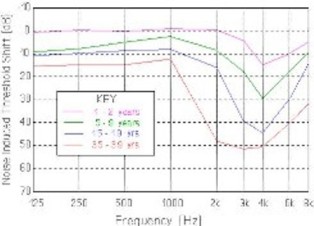
TraumaNoise induced HLProlong exposure to industrial or aircraf noise common progressive notching bilateral at 4000 Hz from audiogram Acoustic traumaSingle sharp sound of high intensity produce sudden unilateral permanent or temporary high frequency SHNL
Meniere ‘s diseaseEndolymphatic hydrops Common disorder of endolymphatic labyrinth of inner ear Unknown etiology Fluctuating SHNL, roaring tinnitus, vertigo, sense of fullness in the ear, recruitment and diplacusis Low-pitched frequencies in early stage Unilateral, 30-50 YO Diagnosis :
Management
Surgical treatment
General management
Central origin(Multiple sclerosis)Chronic demyelination & inflammatory disease Interruption of the auditory pathway Various clinical manifestation but the common is sudden unilateral SNHL Recovery days or weeks
Bone disorder : Cochlear otospongiosisUnknown etiology Progressive SNHL Early or middle adult life Positive FHx : stapes fixation Related to the time of onset or degree fixation Typical high tone loss
Neoplesm(acoutic neuroma)Vestibular schwannoma m/c neoplasm -> SNHL (earliest presentation) Incidence 8-10 % of intracranial neoplasm Unilateral slow progressive high frequency loss Dizziness, tinnitus May involve CN V, VII, cerebellar, brain stem X-ray evidence of bone erosion or around IAM Bilateral in von Recklinghausen’s multiple neurofibromatosis Rx : surgery
PresbycusisProgressive, bilateral, symmetrical Degenerative disorder Old aged Sloping high tone loss to flatter audiogram with a loss for all frequency, with variable impairment of speech discrimination
Summarized By Thirayost Nimmanon â´Â ¸ŐĂÂĘ¶ě ąÔÁÁŇąą·ě
|
|
»ĂŃş»Ăا¤ĂŃé§ĹčŇĘŘ´ 15/06/2010
ä´éĂŃşˇŇĂʹѺʹع Web Hosting ¨Ňˇ SPAComputer.com, ThaWang.com |